







The healthcare coding landscape for Medicare Advantage (MA) significantly shifts based on the transition from the V24 to the V28 Hierarchical Condition Category (HCC) risk adjustment model. This evolution profoundly impacts health plans and providers, necessitating an understanding of the changes and their implications. Let’s explore what this shift entails and how organizations can navigate these updates effectively.
Rationale Behind the Changes
The shift to the V28 model is primarily motivated by the need for greater specificity and accuracy in predicting healthcare costs. The V24 model, based on the less specific ICD-9-CM system, lacked the granularity provided by the ICD-10-CM system. Clinically based adjustments were necessary to ensure diagnoses were solid predictors of cost. In addition, the updated model reduces coding differences between Medicare fee-for-service and Medicare Advantage.
The phased rollout of the V28 code set for Medicare Advantage is over three years:
- 2024: 33% V28 / 67% V24
- 2025: 67% V28 / 33% V24
- 2026: 100% V28
What is Changing from V24 to V28 HCC Models?
The V28 model introduces several key changes from the V24 model, driven by the continued efforts to ensure that the risk adjustment models accurately reflect patient health conditions and the associated expenses to health plans and providers.
One of the primary changes for the V28 HCC-CMS model is a significant increase in HCC categories. The payment HCCs have risen from 86 in V24 to 115 in V28 to support better risk stratification and application of hierarchies and RAF leveling. While the count of HCCs has increased, the ICD coverage has decreased as many ICDs were determined to have little impact on the cost of patient care. The V28 model no longer includes 2,047 ICD codes in V24 model and adds only 269 ICD codes (based on the 2024 mid-year final ICD-10 mappings). These changes had high levels of impact on specific disease categories and conditions, including vascular, metabolic, heart, blood, amputation, neurological, diabetes, kidney, psychiatric, and musculoskeletal.
Criteria for Code Removal
The phased rollout of the V28 code set for Medicare Advantage is over three years:
- ICD-10 Clinical Updates: Most removals (2,161 diagnoses, 95%) were due to clinical updates in the ICD-10 system.
- Principle 10 Updates: About 5% of the removals were based on Principle 10, which aims to reduce the model’s sensitivity to coding variations and ensure clinical credibility as cost predictors.
Removal of conditions fell into six categories:
- Subsequent encounter codes (codes ending in D) – initial encounter diagnosis code is more reliable and predictive
- Sequela codes (codes ending in S) – they are nonspecific, which is the payment exclusion rationale
- Drug-induced conditions – often temporary/reversible and are not good indicators of prospective costs
- Complications of medical care – not reliable predictors of future costs
- Principle 10 – excluding these diagnoses reduces the sensitivity of the model to coding variation
- Other – category indicates decisions were made based on a combination of model principles such as clinical meaningfulness and overprediction
Evaluating the Risk Impact by Category
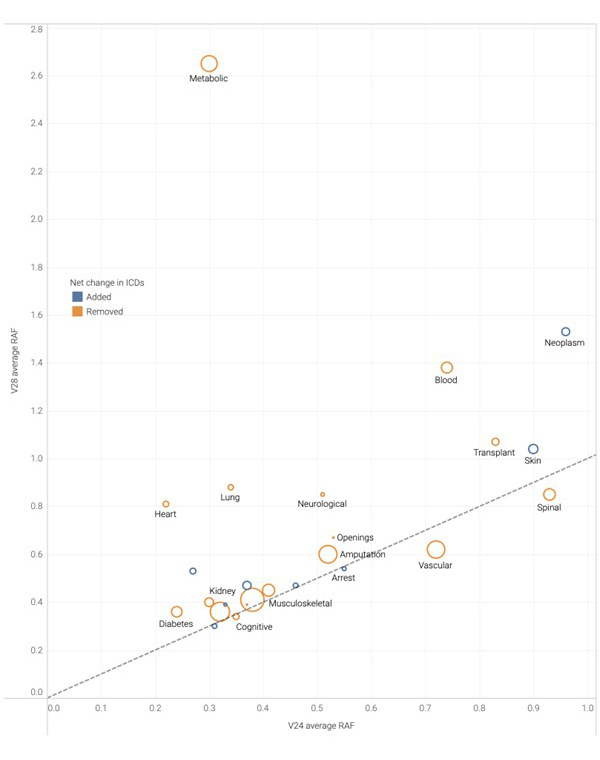
Some interesting patterns emerge when we look at the disease categories and their average RAF per HCC (for aged, non-dual beneficiaries) in both V24 and V28.
- Regardless of the average RAF per HCC, the prevalence of the conditions linked to these HCCs holds more significance. Health plans and providers should analyze patient demographics to identify these emerging trends. Most disease categories show an increase in the average RAF per HCC, except vascular and spinal, which notably decline, and others, like cerebral, cognitive, and arrest, experience a slight drop. It’s important to note that this shift isn’t due to a decrease in the number of HCCs per category; instead, specific categories now have more HCCs with a higher average RAF per HCC.
- Certain disease categories stand out for their rise in average RAF per HCC: Metabolic, Neoplasm, and Blood. These three categories now have more HCCs, indicating CMS focus on greater specificity. For instance, in the Neoplasm category, metastatic cancer was previously counted as a single HCC (8) in V24. With V28, there are now two distinct HCCs for metastatic cancer: one affecting the bone and the other for lung, liver, and brain. CMS recognizes rare diseases such as lysosomal storage disease and various endocrine conditions within the Neoplasm category. Moreover, sickle cell disorders and immunodeficiency-related blood disorders fall under the Blood category, showing the most notable rise in RAF per HCC.
Analyzing V24/V28 ICD Coding Patterns
Looking at early analysis from our health plans and providers, we noticed that the mapped ICDs respective to V24 and V28 HCCs had different value impacts on different disease categories. The difference in the coding patterns and the selected underlying ICDs is the reason behind the discrepancy.

The impact of V24/V28 will vary depending on the disease prevalence in your population. Take a distribution of your HCCs between V24/V28 for ICD-10. Also, provider education on ICD coding will be essential to ensure specificity is captured.
Example of Model Impact
Consider a 65-year-old male with diabetes, peripheral vascular disease (PVD), congestive heart failure (CHF), and protein-calorie malnutrition.
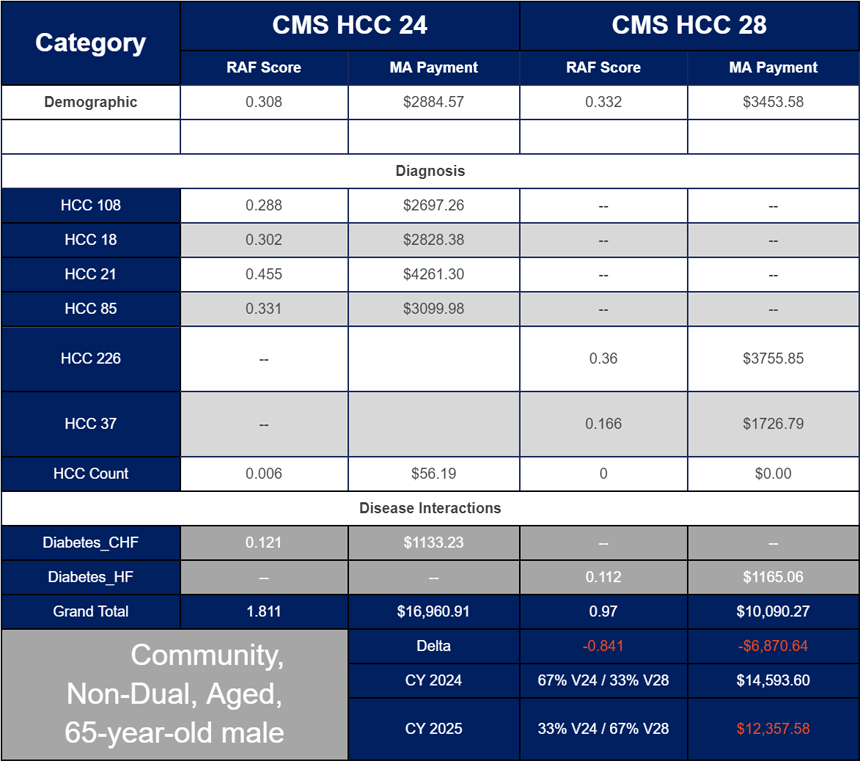
Under the V24 model, this patient would receive separate HCCs and risk adjustment factor (RAF) scores for each condition, resulting in higher overall payments. In the V28 model, conditions like protein-calorie malnutrition and separate PVD no longer contribute to additional HCCs or RAF scores, leading to a lower overall payment. This example underscores the importance of understanding the new mappings and their financial implications.
Recommendations to Navigate the V28 Model
Health plans and providers must adapt to the new normal and have a strategy to navigate the shift to the V28 model. Here are recommendations for health plans and providers to support your risk adjustment program in managing two models.
Health Plans
- Understand the clinical, operational, and financial impact of the V28 model to make data-driven decisions about your risk adjustment strategy.
- Update your suspecting chase logic to acquire relevant patient charts.
- Work with technology partners with experience who can manage V24/V28 models in their analytics and workflows.
- Explore proactive risk adjustment approaches with payer-provider collaboration with data sharing and consider payer-sponsored prospective risk adjustment programs.
Providers
- Educate providers on coding guidelines based on the V28 implications.
- Leverage technology solutions that present recaptured/suspected conditions based on V24/V28 at the point of care.
- Ensure complete, accurate coding and documentation before claims submission.
- Implement claim holds to review new V28 codes before claims submission.
Conclusion
The transition to the V28 HCC model is a significant evolution of the CMS-HCC Model for MA, aimed at enhancing cost prediction accuracy and clinical relevance. This shift necessitates a proactive approach to learning and adaptation for health plans and providers. Staying informed and utilizing technology can help them navigate these changes effectively, ensuring precise and comprehensive documentation of patient conditions.
As the V28 model is progressively rolled out over the next two years, payers and providers must work together and adapt to these changes to successfully oversee their risk adjustment program. The primary goal is to enhance the quality and effectiveness of healthcare delivery.
If you have questions about navigating the V28 model for your organization, please contact us for help with your risk adjustment strategy.